Quick answer: can knee pain be treated without surgery?
Yes, many cases of knee pain do not require surgery. Non-surgical knee pain treatment options include physiotherapy, weight management, anti-inflammatory medication, knee braces, steroid or hyaluronic acid injections, and PRP therapy.
- 1Approximately 80 to 90% of patients with early knee arthritis can be managed without surgery when treatment begins early.
- 2Surgery is considered only when these treatments fail to provide adequate relief over 3 to 6 months.
- 3Bone-on-bone contact alone doesn't necessarily mean surgery is the only path forward.
Most people who come to see Dr. R.P. Singh at Medinity Hospital are not looking for surgery. They are looking for someone to tell them honestly whether they need it. For many patients in Lucknow with knee pain, the honest answer is no, not yet.
Patients come from across Lucknow, including Gomti Nagar, Indira Nagar, Aliganj, Jankipuram, Hazratganj, Alambagh, Mahanagar, Ashiyana, and Chinhat, as well as from Sitapur, Hardoi, Barabanki, Raebareli, Kanpur, and Unnao. Many have been told by a local clinic or general physician that they need surgery. At Medinity Hospital's orthopaedic OPD in Gomti Nagar, a proper assessment often reveals that surgery can be safely postponed, or avoided entirely, with the right non-surgical programme.
Which knee pain symptoms can be treated without surgery?
Before discussing treatment options, it helps to understand which symptoms are typically manageable without surgery and which are warning signs that something more serious may be happening. This table is one of the most common reference points in Dr. R.P. Singh's OPD at Medinity Hospital, Lucknow:
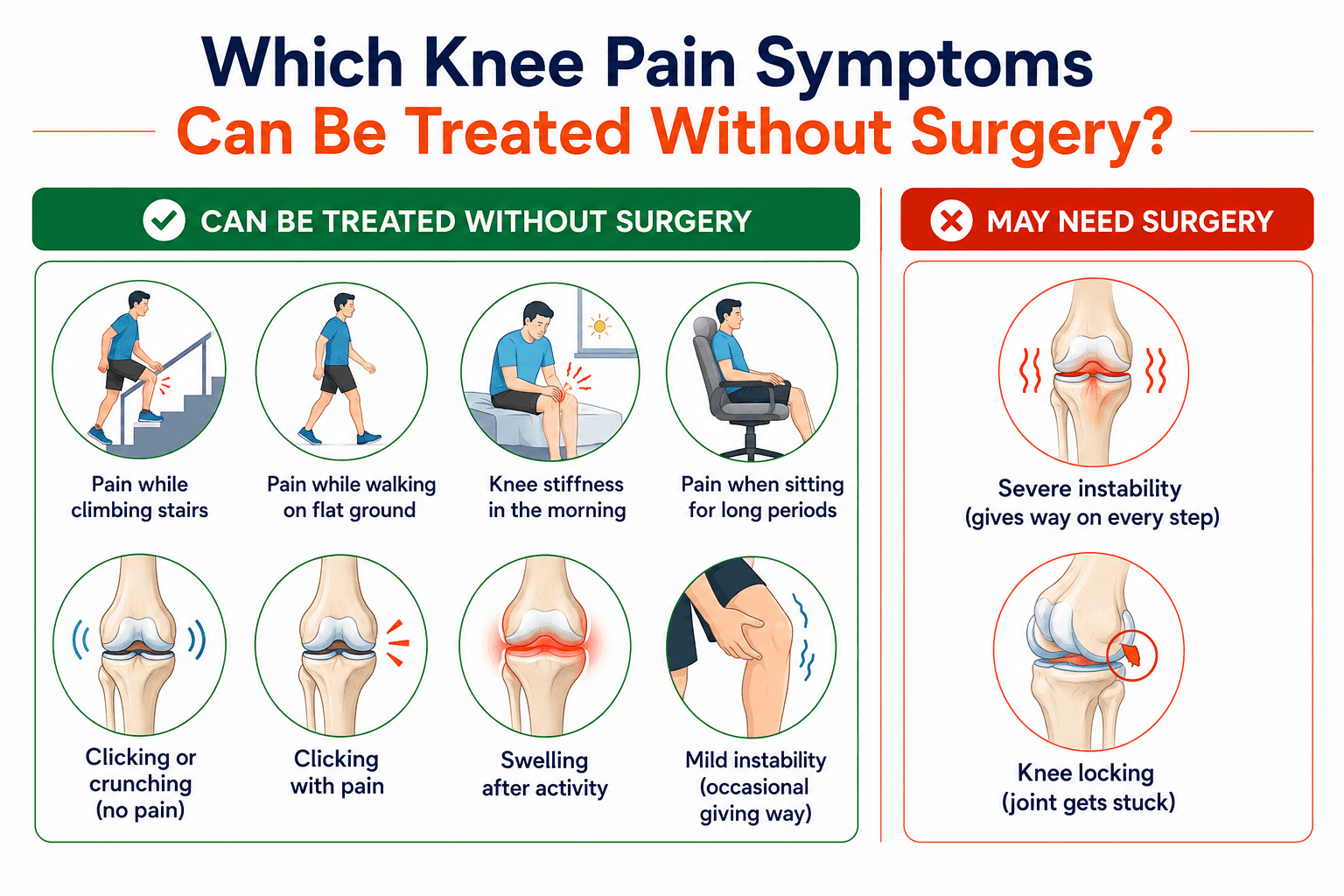
Pain while climbing stairs and morning stiffness are the two most common symptoms patients in Lucknow present with, and both almost always respond to non-surgical treatment in the early to moderate stages. Surgery for these symptoms is rarely indicated unless X-ray confirms advanced bone-on-bone disease and conservative treatment has genuinely failed.
Consultation
Not sure if your symptoms need surgery?
Book an honest first assessment with Dr. R.P. Singh at Medinity Hospital.
CP-221, Hahnemann Medinity Hospital Road, Gomti Nagar, Lucknow 226010 · Walk-in OPD · 24/7 emergency
What causes knee pain that does not need surgery: 4 common conditions
Early to moderate osteoarthritis (Grades 1 to 3)
Morning stiffness, aching after walking, clicking, pain on inner or outer side of knee.
Physiotherapy, weight management, and appropriate injections can control symptoms for months to years. Grade 1 and 2 OA almost never needs surgery if treated consistently.
Patellofemoral pain (kneecap pain)
Pain under or around the kneecap, worse on stairs, getting up from a chair, or after sitting for long periods.
Responds very well to targeted quad and hip strengthening physiotherapy. Surgery is rarely needed.
Meniscus irritation (without mechanical locking)
Knee clicking, occasional mild locking, pain on bending. Swelling after activity.
A 2013 NEJM METEOR trial showed physiotherapy produced equivalent outcomes to arthroscopic surgery for degenerative meniscus tears. Non-surgical treatment should always be tried first.
Grade 1 and 2 ligament sprains
Pain and swelling within 24 to 48 hours of injury. Mild instability. Tenderness over ligament.
Physiotherapy, bracing, and progressive loading over 4 to 12 weeks. Surgery reserved for complete Grade 3 ACL tears in active patients wanting to return to sport.
Bone-on-bone contact on X-ray does not automatically mean surgery. Dr. R.P. Singh regularly sees patients in Lucknow who have been told they need knee replacement based on an X-ray alone, but who still have significant improvement available from non-surgical management. The decision to operate depends on X-ray findings plus symptom severity plus failed conservative treatment together, not on X-ray findings alone.
Non-surgical treatment options: physiotherapy, injections, bracing and weight management
Non-surgical treatment is most effective when several approaches are combined rather than tried one at a time:
All stages of knee arthritis, patellofemoral pain, ligament sprains. First-line treatment in most orthopaedic guidelines.
Overweight patients with any stage of arthritis.
Short-term symptom control at all stages.
Unicompartmental arthritis with mild varus or valgus deformity. Ligament sprain support.
Chronic stiffness, morning aching (no swelling).
Acute swelling, inflammation, post-exercise soreness.
Optional supportive therapy in any stage.
Use Heat When:
- Stiff but not swollen
- Chronic dull aching pain
- Morning stiffness before exercise
Heat relaxes muscle, improves blood flow.
Use Ice When:
- Visibly swollen
- Red, warm, or inflamed
- After exercise or activity
Never apply heat to an actively inflamed joint.
When does non-surgical treatment stop being enough? The 5 clear signs
Night pain that wakes you from sleep
What it means: Rest pain indicates arthritis has progressed beyond mechanical load-related inflammation to persistent advanced inflammatory disease.
Next step: Surgical assessment is appropriate if this is present after 3 to 6 months of consistent conservative treatment.
Injections no longer providing adequate relief
What it means: Steroid injections that previously lasted 4 to 6 months now last weeks or give no benefit.
Next step: When injections fail at this level, cartilage loss is typically so advanced that anti-inflammatory treatment cannot address the structural problem.
X-ray shows bone-on-bone contact or significant deformity
What it means: Joint space has narrowed completely or a significant angular deformity has developed.
Next step: The three-part threshold: bone-on-bone plus significant symptoms plus failed conservative treatment together justify surgical evaluation.
Cannot walk 500 metres without stopping
What it means: Significant functional limitation affecting independence and daily activities.
Next step: Loss of walking ability at this level, after genuine conservative treatment, meets the quality-of-life threshold for surgical consideration.
Pain affecting sleep, social life, and mental wellbeing consistently
What it means: The psychological burden of uncontrolled chronic knee pain is a clinical concern in its own right.
Next step: When pain has reduced quality of life across multiple domains and non-surgical treatment cannot restore adequate function, surgery genuinely improves outcomes.
If you believe these signs apply to your situation, our detailed guide on total knee replacement in Lucknow explains the surgical options (or partial knee replacement), costs, and recovery timeline.
Consultation
Not sure if you have reached the surgical threshold?
Book an evaluation with Dr. R.P. Singh at Medinity Hospital.
CP-221, Hahnemann Medinity Hospital Road, Gomti Nagar, Lucknow 226010 · Walk-in OPD · 24/7 emergency
PRP and hyaluronic acid injections: do they actually work? An evidence-based answer
PRP and hyaluronic acid injections are increasingly discussed for knee arthritis. Here is what the 2024 to 2025 published clinical evidence shows:
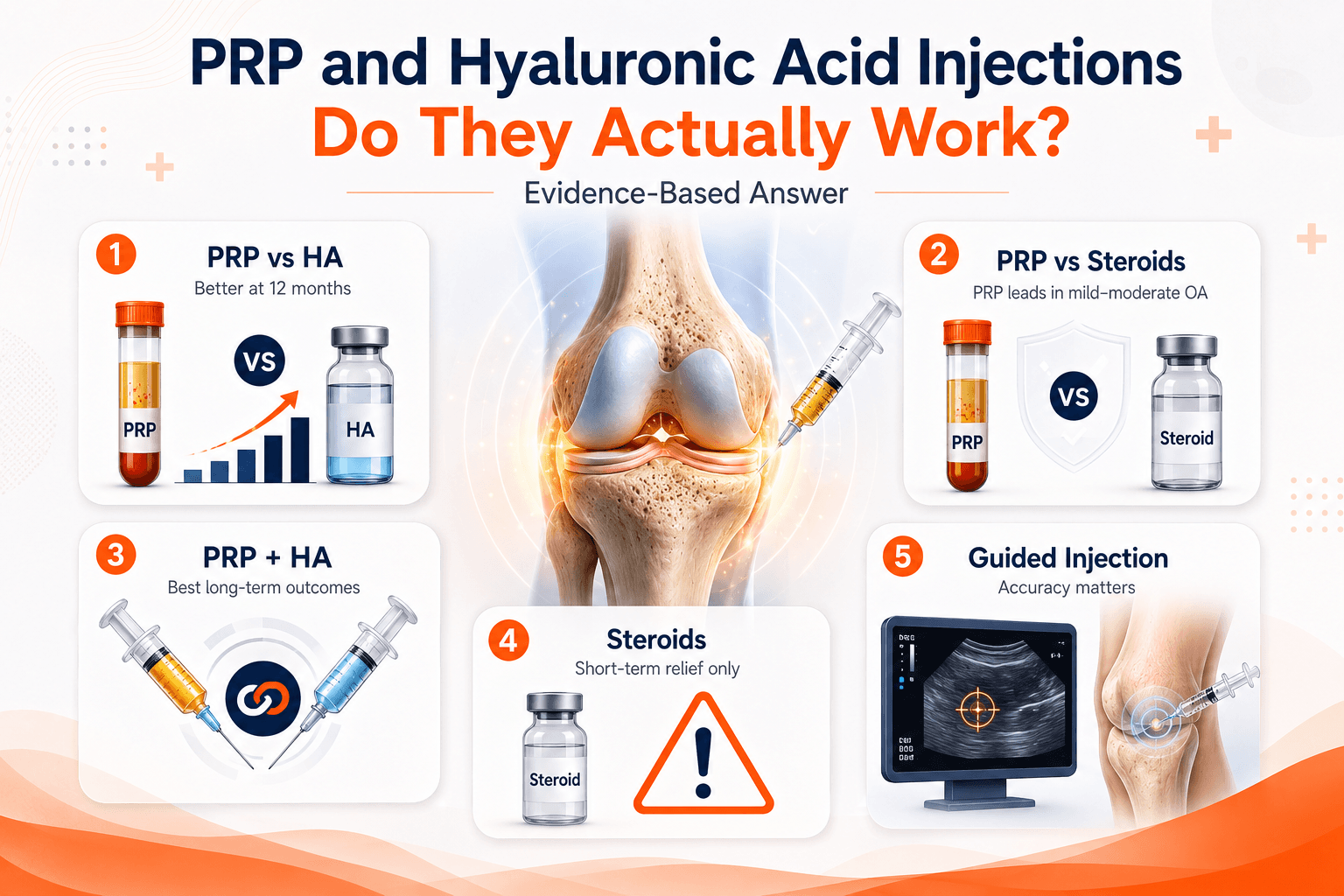
A 2024 meta-analysis of 15 double-blind RCTs including 1,632 patients found PRP produced significantly lower pain scores and better WOMAC function scores at 12 months compared to HA injections.
A 2025 comprehensive review of 40 high-quality studies confirmed leukocyte-poor PRP superior to both corticosteroids and HA in mild to moderate OA (Grades 1 to 3).
A 2024 meta-analysis of 11 RCTs (1,023 patients) found PRP plus HA combination therapy produced superior long-term outcomes compared to PRP alone with a lower adverse event rate.
Repeated cortisone injections cause chondrocyte (cartilage cell) death over time. AAOS guidelines reflect concern about frequent repeat steroid injections in the same joint. Steroids useful short-term for acute flares but should not be used repeatedly as long-term management.
Blind injections without ultrasound guidance have accuracy rates as low as 55% in published studies. Ultrasound guidance virtually eliminates missed injections. All injections at Medinity Hospital are administered under imaging guidance where clinically appropriate.
PRP injection: quick decision guide
- Mild to moderate OA (Grades 1 to 3): strong evidence of benefit
- Injections failing: PRP gives more durable results when HA/steroids fail
- Younger patients: wanting to delay surgery and slow arthritis progression
- Steroid alternative: patients not suitable for or wanting to avoid steroids
- Grade 4 (bone-on-bone): PRP less effective when cartilage is completely gone
- Antiplatelet medication: patients on aspirin or clopidogrel need medical clearance
- Active joint infection: injection contraindicated
What happens at a first orthopaedic consultation at Medinity Hospital
Many patients in Lucknow delay seeing an orthopaedic surgeon because they fear the first appointment will immediately lead to surgery. It does not. Here is exactly what a first consultation involves:
1. History
Dr. R.P. Singh asks about your knee pain: when it started, what makes it worse, what has been tried, and how it affects daily life. Bring prescriptions or records.
2. Physical examination
Knee examined for swelling, range of motion, tenderness, ligament stability, and specific condition signs. Takes 5 to 10 minutes.
3. Imaging review
Existing X-rays or MRI are reviewed. If none, a standing weight-bearing X-ray is arranged at Medinity's NABL-accredited diagnostics centre on the same visit.
4. Diagnosis and explanation
Dr. R.P. Singh explains what he has found in plain language: what the condition is, how serious it is, and what the realistic options are.
5. Treatment plan
For most first consultations, a non-surgical plan is recommended in writing. Surgery is only discussed if the clinical and imaging picture clearly justifies it.
How to know if your knee pain needs an MRI or an X-ray first
X-ray (standing, weight-bearing)
What it shows best: Bone structure, joint space width, bone spurs, alignment and deformity.
When to use it first: First investigation for any suspected arthritis. Standing view essential. X-ray is usually enough to diagnose and stage arthritis in most patients.
MRI
What it shows best: Soft tissues: cartilage detail, meniscus, ligaments, tendons, bone marrow. Detects early AVN.
When to use it first: Use when: ligament tear suspected after injury, meniscus surgery is being considered, X-ray is normal but pain is significant, AVN suspected.
Many patients in Lucknow spend ₹5,000 to ₹10,000 on an MRI before seeing a doctor, when a ₹300 standing X-ray would have answered the clinical question. An MRI before a basic X-ray for straightforward arthritis adds cost without changing the management plan. Ask your doctor which investigation is needed first.
What happens after your first visit? A typical non-surgical patient journey
For patients starting non-surgical knee pain treatment at Medinity Hospital, Gomti Nagar, Lucknow, here is what the pathway typically looks like:
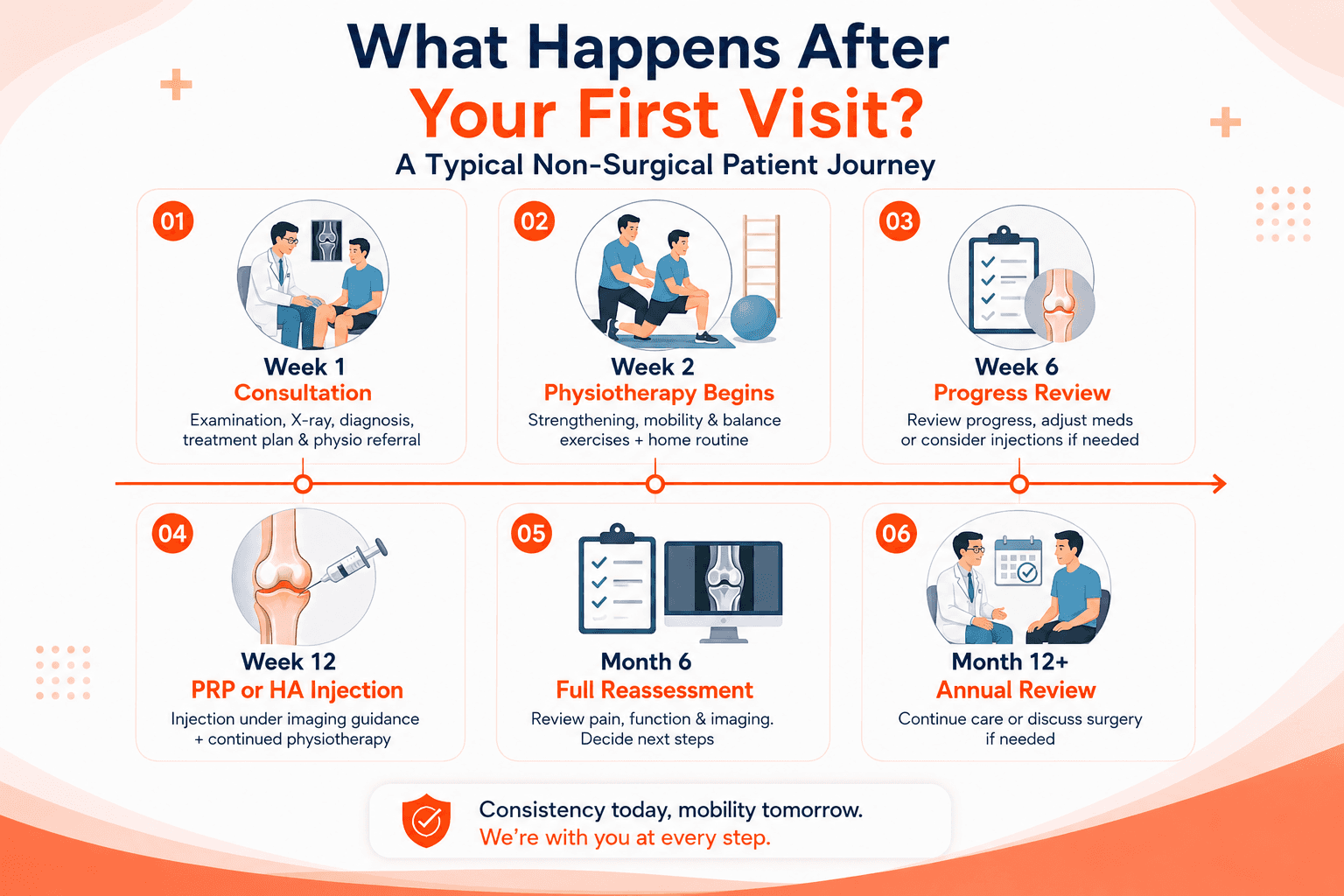
A genuine non-surgical trial takes time. You cannot declare that "physiotherapy didn't work" after three days of exercises. Here is the typical timeline for a patient starting conservative management for knee arthritis at Medinity Hospital:
Week 1: Consultation
Clinical examination, weight-bearing X-ray, diagnosis. Written treatment plan. Physiotherapy referral arranged at Medinity's integrated physio department in Gomti Nagar.
Week 2: Physiotherapy begins
Formal physiotherapy programme starts: quad and VMO strengthening, hip abductor work, proprioception training. Home exercises prescribed for daily practice.
Week 6: Progress review
Dr. R.P. Singh reviews your pain, function, and physiotherapy progress. Medication adjusted if needed. If improvement is insufficient, injections are considered.
Week 12: PRP or HA injection (if needed)
For patients not adequately responding to physiotherapy alone, PRP injection is offered under imaging guidance at Medinity Hospital, Lucknow. Physiotherapy continues alongside.
Month 6: Full reassessment
Comprehensive review of pain, function, walking ability, quality of life, and updated imaging if appropriate. Decision: continue conservative management, adjust treatment, or begin surgical evaluation if the 5 thresholds have been reached.
Month 12+: Annual review
Most patients at this stage are managing well on a non-surgical programme. For those who have progressed to bone-on-bone disease despite optimal treatment, surgical discussion is initiated.
This is a typical pathway, not a fixed protocol. Some patients improve significantly at week 6 and need nothing further for 12 to 18 months. Others need more frequent review. Dr. R.P. Singh tailors the timeline to each patient's response, not to a fixed schedule.
Consultation
Want a second opinion on your knee pain?
Bring your MRI and X-rays to Dr. R.P. Singh at Medinity Hospital, Gomti Nagar. Get a clear, written assessment of whether surgery is genuinely necessary.
CP-221, Hahnemann Medinity Hospital Road, Gomti Nagar, Lucknow 226010 · Walk-in OPD · 24/7 emergency
Non-surgical knee pain self-management: what helps and what to avoid
What Genuinely Helps
- Walk on flat, even surfaces daily (30 mins if pain allows)
- Stationary cycling or swimming 3 to 5 times per week
- Straight leg raises 3 sets of 10, 3 days per week
- Ice the knee for 15-20 mins after activity if it swells
- Reduce sugar, fried food, and alcohol intake
- Use a raised toilet seat to avoid deep knee bending
What To Avoid
- Running or jogging on hard roads or pavements
- Deep squats, lunges, or heavy leg press at the gym
- Sitting cross-legged or using Indian-style squat toilets
- Applying heat to a swollen or inflamed knee
- Wearing a knee brace constantly without physiotherapy
Cost of non-surgical knee pain treatment in Lucknow: what to expect
Cost is one of the most common questions at the Medinity Hospital orthopaedic OPD. Here is a transparent framework for what non-surgical knee pain treatment costs in Lucknow:
Do not compare hospitals on price alone for injection therapy. PRP injected without ultrasound guidance has a 45% miss rate in published studies, meaning the injection misses the knee joint entirely. A blind PRP injection at a lower cost is not a saving. It is an ineffective procedure. At Medinity Hospital, Gomti Nagar, Lucknow, all injections are administered under imaging guidance where clinically appropriate.
Transparent Pricing at Medinity Hospital
Medinity Hospital provides a transparent itemised cost for all orthopaedic procedures before any treatment is started. To understand the cost of your specific treatment plan, call +91 94540 99331 or book a consultation with Dr. R.P. Singh at Gomti Nagar, Lucknow.
Why patients trust Medinity Hospital for non-surgical knee pain treatment in Lucknow
- Dr. R.P. Singh: MS Ortho (Gold Medalist), Fellowship Joint Replacement, USA and Germany
- 20+ years of orthopaedic practice, 2,000+ joint replacement surgeries performed
- Non-surgical management always considered first: no pressure to operate
- PRP and injection therapy administered under imaging guidance
- NABH-accredited hospital | NABL-accredited diagnostics
- Integrated physiotherapy and rehabilitation department on the same campus
- 4.8-star rating from 246+ verified Google reviews
Help centre
Frequently asked questions
Very mild, short-term knee pain from overuse or a minor sprain can sometimes resolve on its own with rest, ice, and reduced activity over 2 to 4 weeks. However, knee arthritis does not heal on its own because cartilage has no blood supply and cannot regenerate. If knee pain has persisted for more than 4 to 6 weeks, has not improved with rest, or is affecting daily activities, it needs professional assessment. Waiting indefinitely for arthritis to resolve on its own allows the condition to progress and makes future treatment more complex.
After a minor knee sprain or injury, stairs with a handrail are usually manageable from day 1 as long as pain is tolerable. After a PRP injection, most patients are advised to avoid strenuous stair climbing for 1 to 2 weeks while the platelet activity phase completes. After a cortisone injection, there are no activity restrictions. After a hyaluronic acid injection, light stair use is fine from the same day. For patients with moderate to severe arthritis, stairs remain painful regardless of injection therapy until the underlying disease is addressed.
Light stair climbing is generally acceptable within a few days of PRP injection, as long as it is not strenuous. Most physiotherapists and orthopaedic specialists recommend avoiding heavy loading of the knee including running, jumping, and prolonged stair climbing for 1 to 2 weeks after PRP to allow optimal platelet activation and inflammatory response. Walking on flat ground is fine from the same day. Dr. R.P. Singh will give specific activity guidance based on your injection protocol at Medinity Hospital, Lucknow.
Yes. Excess body weight increases the mechanical load through the knee joint significantly. Even without any cartilage damage, the compressive force on the knee during walking can cause joint inflammation, synovitis (swelling of the joint lining), patellofemoral pain, and gradual cartilage stress. Every kilogram of body weight puts approximately 4 kg of force through the knee joint during normal walking. This means a 10 kg reduction in body weight reduces knee loading by approximately 40 kg per step, which is clinically significant. Weight management is treatment, not just lifestyle advice.
Yes, stationary cycling is one of the best exercises for knee arthritis and is specifically recommended at Medinity Hospital for orthopaedic patients. Cycling strengthens the quadriceps without the impact loading of walking or running, maintains joint range of motion, and improves cardiovascular fitness. Use a high seat position so the knee only bends to 90 degrees or less. Keep resistance low initially. Outdoor cycling on uneven road surfaces is less ideal because of the unpredictable load. Swimming and hydrotherapy are the other two consistently recommended low-impact activities.
Vitamin D deficiency can contribute to musculoskeletal pain including knee pain, though it does not directly cause arthritis. Vitamin D is important for bone density and muscle function. Deficiency is extremely common in India due to indoor lifestyles and dietary factors. Low vitamin D levels can worsen the pain experienced from existing arthritis and are associated with increased risk of bone and joint pain. A simple blood test at Medinity's NABL-accredited lab can check your vitamin D level. Supplementation is safe, inexpensive, and should be considered as part of any comprehensive non-surgical knee management plan.
Yes, in many cases. Early to moderate osteoarthritis (Grades 1 to 3), patellofemoral pain, meniscus irritation without a mechanical tear, and Grade 1 to 2 ligament sprains all respond well to non-surgical treatment. The combination of physiotherapy, weight management, appropriate injections, and activity modification can control symptoms for months to years. Surgery is reserved for patients where this has been genuinely tried and the condition has progressed beyond what conservative management can address.
The standard clinical guideline is 3 to 6 months of consistent, properly applied conservative treatment. This means formal physiotherapy with a qualified therapist, not just occasional home exercises, combined with weight management and appropriate medication. If after this period pain is still significantly affecting your daily life, surgical evaluation at Medinity Hospital, Lucknow, is appropriate.
For mild to moderate knee osteoarthritis (Grades 1 to 3), PRP injections are supported by strong evidence. A 2024 meta-analysis of 15 double-blind RCTs including 1,632 patients found PRP produced significantly better pain relief and functional outcomes than hyaluronic acid at 12 months ScienceDirect, 2024. A 2025 review of 40 high-quality studies confirmed PRP superiority over both corticosteroids and HA in mild to moderate OA PMC 2025. PRP is less effective in Grade 4 (bone-on-bone) disease.
Steroid injections are safe and effective for short-term pain relief and acute inflammatory flares. However, growing evidence shows that repeated corticosteroid injections accelerate cartilage cell death. At Medinity Hospital, cortisone injections are used selectively for acute flares, not as regular long-term management. If injections are no longer providing adequate relief, PRP or surgical evaluation is more appropriate.
Safe exercises include walking on flat surfaces, stationary cycling (low resistance), swimming, and hydrotherapy. Exercises to avoid include running on hard surfaces, deep squats, jumping, and heavy resistance leg training. Even if you cannot swim, walking in waist-deep water reduces joint load by approximately 50% compared to land-based walking. Strong quads protect the knee better than any brace.
Offloading braces can be helpful for unicompartmental arthritis and mild varus or valgus deformity. However, braces should not be worn constantly or as a substitute for physiotherapy. Prolonged brace dependence weakens the muscles that naturally support the knee, making the joint more vulnerable when the brace is removed.
Yes. Deep knee flexion including sitting cross-legged and using Indian-style squat toilets places significantly higher load on the knee joint than normal sitting. For patients with Grade 2 arthritis or above, these positions accelerate cartilage wear. Switching to a raised western-style toilet seat is one of the simplest and most effective lifestyle modifications for knee arthritis in Lucknow.
Walking is good for knee arthritis when done correctly on flat, even surfaces with supportive footwear. Regular walking maintains muscle strength and keeps the joint lubricated. Running and walking on uneven or hard surfaces should be avoided in moderate to severe arthritis. Stop if pain significantly worsens during the walk.
See a doctor promptly if: the knee is visibly swollen after injury, you cannot bear weight, you heard a pop or crack at the moment of injury, the knee locks and cannot be straightened, or pain has not improved after 4 to 6 weeks of rest and basic self-care. Persistent knee pain beyond 6 weeks should always be assessed professionally.
Yes, significantly. Each kilogram of body weight reduction reduces knee loading by approximately 4 kg during walking. A 5 kg loss reduces knee loading by 20 kg per step. Studies show that patients with mild to moderate arthritis who achieve meaningful weight loss frequently experience pain relief equivalent to or greater than injection therapy. Weight loss is the most cost-effective and durable non-surgical intervention available.
No. Many people over 40 have MRI findings described as meniscus tears or cartilage changes that cause no symptoms. Conversely, some patients with severe pain have MRI findings that appear mild. An MRI alone cannot determine whether surgery is needed. It must be interpreted alongside clinical examination, symptoms, and a weight-bearing X-ray.
Yes. Medinity Hospital, Gomti Nagar, Lucknow, offers PRP injection therapy as part of its orthopaedic non-surgical programme under Dr. R.P. Singh's supervision. All injections are administered under imaging guidance where clinically appropriate. To book a consultation and discuss whether PRP is right for your condition, call +91 94540 99331.
Physiotherapy for knee pain specifically targets VMO activation (the inner quad that most arthritis patients cannot engage), hip abductor strengthening, proprioception improvement, and movement pattern correction. General exercise does not address these specific deficits. A physiotherapist-guided programme produces significantly better outcomes than general exercise advice alone. Medinity Hospital's physiotherapy department is integrated with the orthopaedic clinic at the same Gomti Nagar campus.
PRP injection costs in Lucknow typically range from ₹8,000 to ₹20,000 per injection at quality centres, depending on the concentration protocol used. PRP is not covered by most insurance policies in India. However, a well-administered PRP injection under imaging guidance that provides 12 months of pain relief is cost-effective compared to repeated steroid injections that provide 6 to 8 weeks of relief at ₹1,000 to ₹2,000 each, plus the accumulated cartilage damage risk. Medinity Hospital provides a transparent cost estimate before any procedure.

About the author
Dr. R.P. Singh
MS Ortho (Gold Medalist) · Fellowship Joint Reconstruction (USA, Germany) · Senior Orthopaedic Surgeon
- 20+ years experience
- 2,000+ surgeries
- Partial & total knee replacement
Dr. R.P. Singh leads orthopaedics at Medinity Hospital, Gomti Nagar. He specialises in both joint preservation and replacement, bringing international, evidence-based surgical standards to Lucknow.
View full profile & credentials