Quick answer: what is frozen shoulder and how is it treated?
Frozen shoulder (adhesive capsulitis) is a painful condition where the shoulder capsule thickens and tightens, severely restricting movement. It progresses through 3 stages: freezing (pain-dominant, 10 to 36 weeks), frozen (stiffness-dominant, 9 to 12 months), and thawing (gradual recovery, 12 to 42 months). Treatment is stage-specific and includes corticosteroid injections (Stage 1), physiotherapy and hydrodilatation (Stage 2), and arthroscopic capsular release for resistant cases. Diabetes patients face 2 to 3 times higher risk and more severe disease. The condition affects 2 to 5% of adults and is fully treatable in the vast majority of cases.
If you have been struggling to lift your arm above your head, cannot reach behind your back, or wake up at night because of shoulder pain, you may have frozen shoulder. It is one of the most commonly misdiagnosed and mistreated conditions in orthopaedic practice, partly because it looks different at different stages.
Dr. R.P. Singh, Senior Orthopaedic Surgeon at Medinity Hospital, Gomti Nagar, Lucknow, regularly treats patients from across Lucknow, including Hazratganj, Alambagh, Indira Nagar, Aliganj, Jankipuram, Chinhat, and Mahanagar, as well as from Sitapur, Hardoi, Barabanki, Raebareli, and Kanpur who have been living with a frozen shoulder for months before getting the right diagnosis. This article explains what frozen shoulder is, how to recognise your stage, what each investigation tells us, what treatment is most effective, what it costs in Lucknow, and how to prevent it.
What is frozen shoulder and why do doctors call it adhesive capsulitis?
Your shoulder joint is surrounded by a thick envelope of tissue called the joint capsule. In frozen shoulder (adhesive capsulitis), this capsule becomes inflamed and progressively thickens and contracts. As it tightens, movement becomes restricted and painful.
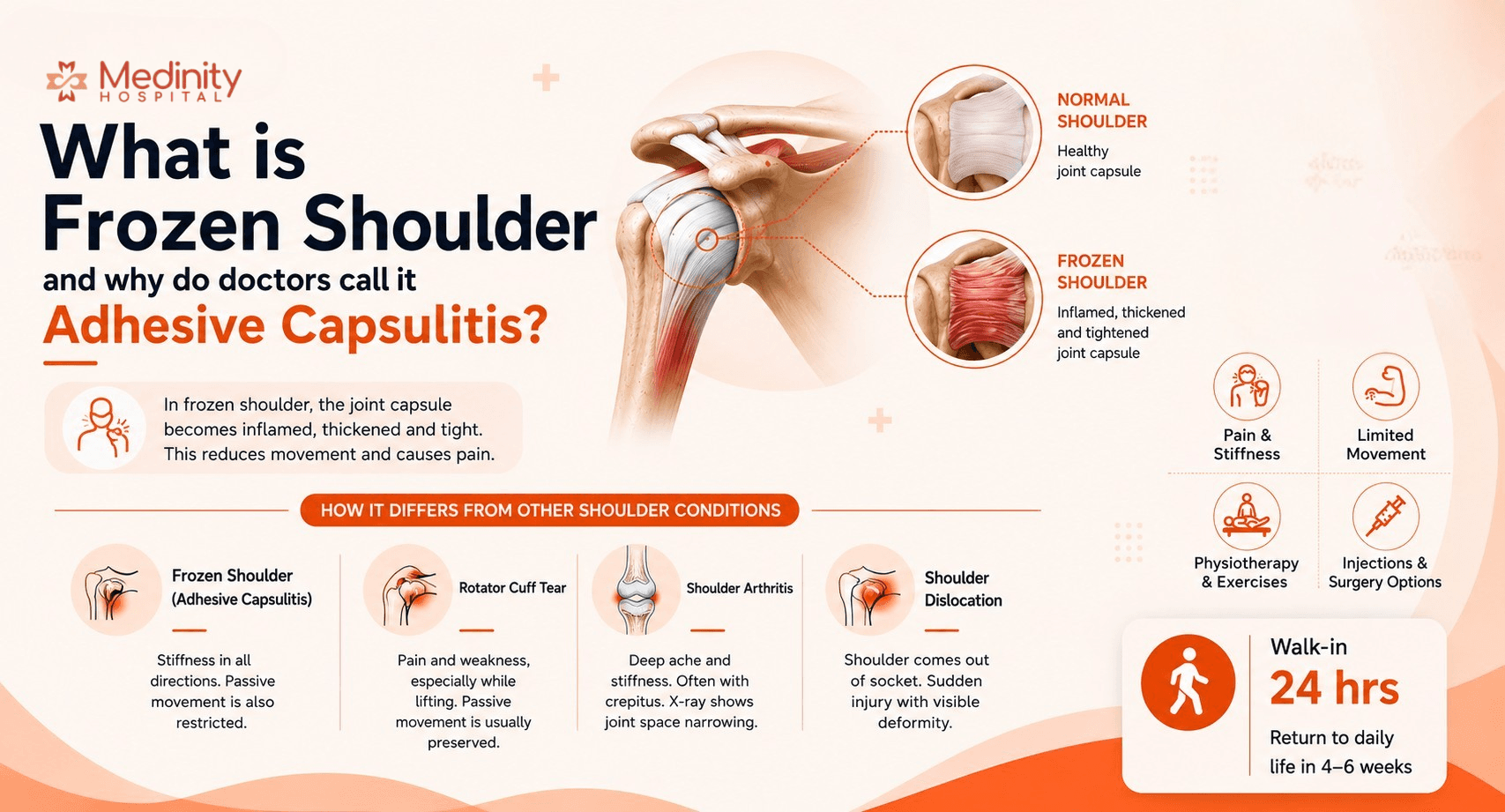
The single most important clinical sign: when a doctor or physiotherapist tries to move your arm and it is equally restricted whether you help or not, that is adhesive capsulitis until proven otherwise. This loss of passive movement distinguishes frozen shoulder from rotator cuff tears, where passive movement is usually preserved.
Joint capsule thickens and contracts
Pain and progressive stiffness in all directions
Passive movement restricted equally as active movement
Shoulder tendons
Pain and weakness, especially lifting
Passive movement usually preserved. Weakness is dominant.
Cartilage and bone of the joint
Deep aching, crepitus, stiffness after rest
X-ray shows joint space narrowing. Less common than hip or knee.
Ligaments and labrum
Shoulder comes out of socket, immediate deformity
Event-related, structural. May recur if labrum is untreated.
The 3 stages of frozen shoulder: freezing, frozen and thawing and what each feels like
Treatment that helps in Stage 1 can make Stage 2 significantly worse. Understanding your stage is not academic. It determines which treatment is appropriate and what to expect.
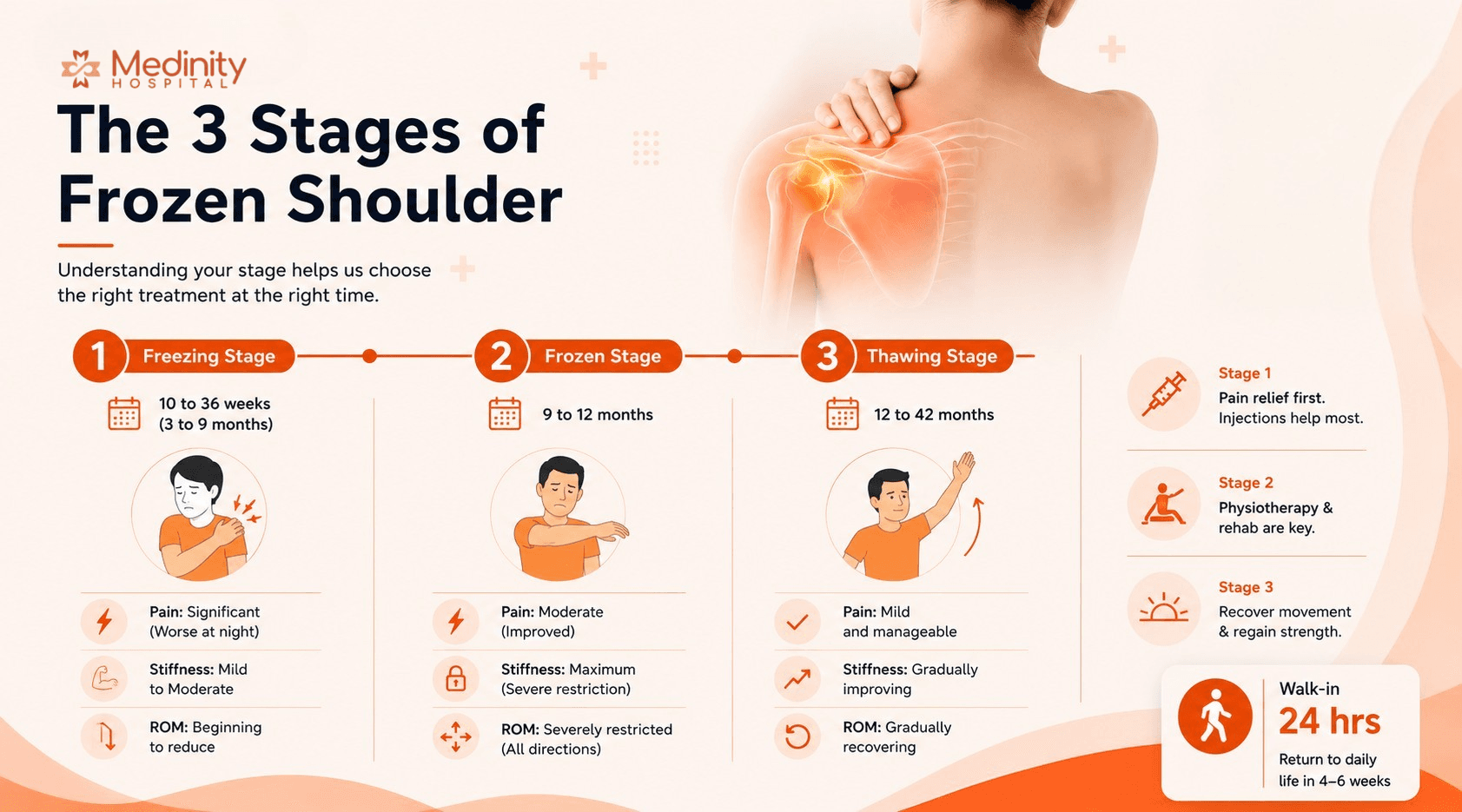
1 Stage 1: Freezing stage
- Typical duration: 10 to 36 weeks (approximately 3 to 9 months)
- Pain level: Significant, often severe. Worse at night. Pain comes before stiffness becomes obvious.
- Stiffness: Mild to moderate. The joint is becoming stiffer but pain dominates.
- Range of motion: Beginning to reduce.
- Best treatment focus: Pain management is the priority. Steroid injections in this stage give the most significant and fastest benefit. Gentle physiotherapy only, not aggressive stretching.
2 Stage 2: Frozen stage
- Typical duration: 9 to 12 months
- Pain level: Less severe than Stage 1. Pain improved but movement is severely restricted.
- Stiffness: Maximum stiffness. Cannot lift arm to shoulder height, cannot rotate outward, cannot reach behind the back.
- Range of motion: Severely restricted in all directions. Passive equally limited as active.
- Best treatment focus: Physiotherapy and rehabilitation at Medinity and hydrodilatation are the cornerstones. Steroid injections have less benefit here than in Stage 1.
3 Stage 3: Thawing stage
- Typical duration: 12 to 42 months
- Pain level: Generally mild and manageable.
- Stiffness: Gradually improving month by month.
- Range of motion: Progressively recovering, though slower in diabetic patients.
- Best treatment focus: Structured physiotherapy to maximise range of motion recovery. Surgery (arthroscopic capsular release) if recovery has stalled beyond 12 to 18 months.
The most common clinical error
Aggressive shoulder stretching in Stage 1 (the freezing stage) makes frozen shoulder significantly worse. Diagnosis and staging by an orthopaedic specialist before starting physiotherapy is critical.
Consultation
Not sure which stage of frozen shoulder you are in? Book an assessment.
CP-221, Hahnemann Medinity Hospital Road, Gomti Nagar, Lucknow 226010 · Walk-in OPD · 24/7 emergency
Who gets frozen shoulder? Risk factors, diabetes, thyroid and why women are more affected
Diabetic patients have a 10 to 20% lifetime incidence, 2 to 3 times higher than the general population. Advanced glycation end-products stiffen the shoulder capsule.
More severe, more resistant to treatment, lasts longer, more likely to affect both shoulders. A 2023 BMJ Open meta-analysis confirmed diabetes as an independent risk factor.
Both hypothyroidism and hyperthyroidism are associated with frozen shoulder (Chuang et al. 2023 meta-analysis).
Unexplained frozen shoulder should prompt thyroid function testing. Treating the thyroid condition may improve treatment response.
Peak incidence in the mid-50s. The shoulder capsule undergoes collagen changes from the mid-40s.
Frozen shoulder is rare under 40 and uncommon over 65.
Women affected at 3.38 versus 2.36 per 1,000 person-years. Perimenopausal hormonal changes may play a role in capsular fibrosis.
Women account for slightly more than half of all frozen shoulder cases in epidemiological studies.
Any period of shoulder immobilisation can trigger the condition.
Post-injury and post-surgical frozen shoulder is common and preventable with early physiotherapy and range-of-motion exercises.
Immobilising the shoulder for another arm injury (wrist fracture, elbow surgery) can trigger frozen shoulder.
Patients in slings should perform regular shoulder range-of-motion exercises unless specifically contraindicated.
Consultation
Have diabetes and shoulder pain? Book an early assessment before the condition progresses.
CP-221, Hahnemann Medinity Hospital Road, Gomti Nagar, Lucknow 226010 · Walk-in OPD · 24/7 emergency
How is frozen shoulder diagnosed? Clinical examination, X-ray, MRI and blood tests
One of the most important things patients in Lucknow should know: frozen shoulder is a clinical diagnosis. It is made by examining the shoulder, not primarily by imaging. X-rays and MRI are used to rule out other conditions, not to confirm frozen shoulder itself.
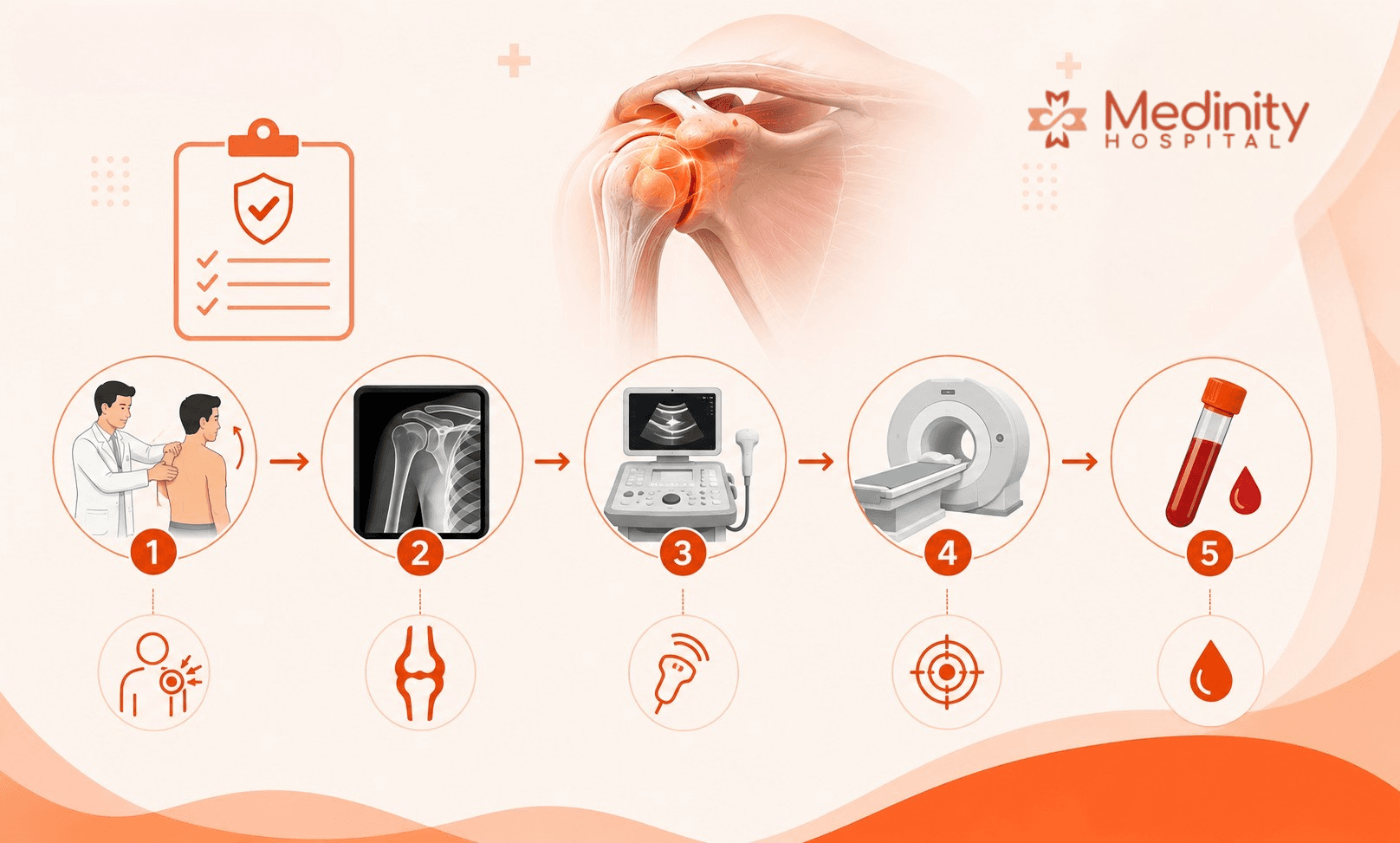
The clinician moves the patient's arm in all directions with the patient relaxed. Tests external rotation with elbow at side, forward flexion, internal rotation.
Equally restricted in active and passive movement in all planes. External rotation with elbow at side is typically the earliest and most restricted movement.
Always the first and most important diagnostic step. Cannot be replaced by imaging.
Bone structure, joint space, bone spurs, deformity.
Usually completely normal. This surprises many patients. A normal X-ray does not mean nothing is wrong. It rules out arthritis and bone pathology, which supports the frozen shoulder diagnosis.
Always done to rule out arthritis, fracture, and bone lesions. Available at Medinity's NABL-accredited diagnostics Medinity Hospital in Gomti Nagar.
Soft tissues, tendons, bursa, joint fluid. Real-time dynamic imaging.
May show thickening of the coracohumeral ligament and posterior capsule. Also useful to guide injections.
Useful when rotator cuff tear needs to be ruled out alongside frozen shoulder. Also used to guide all shoulder injections at Medinity Hospital.
Detailed imaging of all soft tissue structures including cartilage, labrum, tendons, and capsule.
Shows capsular thickening, reduced joint volume, and capsular adhesions in advanced cases. More sensitive than ultrasound for detailed capsular assessment.
Used when the diagnosis is uncertain, when a labral tear or significant rotator cuff pathology needs to be excluded, or when surgery is being planned.
Confirms or rules out diabetes and thyroid disorders, both of which are significantly associated with frozen shoulder.
Not diagnostic for frozen shoulder itself but essential as part of the assessment in any patient without a clear precipitating cause.
Recommended for all patients with frozen shoulder who do not have a clear mechanical trigger. Early identification of diabetes or thyroid disease allows targeted treatment alongside shoulder management.
Dr. R.P. Singh, an expert orthopaedic surgeon in Lucknow at Medinity Hospital, Gomti Nagar, performs a structured shoulder examination at every first appointment. Blood tests for HbA1c and thyroid function are arranged at Medinity's NABL-accredited laboratory on the same visit when indicated. Ultrasound-guided injections are used for both diagnostic accuracy and therapeutic effectiveness.
Frozen shoulder treatment in Lucknow: physiotherapy, injections and when surgery is needed
Treatment must be matched to the stage. Here is the evidence-based framework used at Medinity Hospital, Gomti Nagar, Lucknow:
Stage 1 primarily. Some benefit in early Stage 2.
Steroid injected directly into the shoulder joint under ultrasound guidance. 1 to 2 injections spaced 4 to 6 weeks apart.
Strongest evidence for pain reduction in Stage 1. Benefit is primarily on pain, not long-term ROM recovery.
Stage 2 (most responsive). Stage 3 (maximising recovery). Stage 1 (gentle only).
Structured programme: pendulum exercises, capsular mobilisation, progressive stretching. Aggressive stretching in Stage 1 worsens the condition.
Supervised physiotherapy significantly outperforms home exercises alone in published studies for Stage 2.
Stage 2 and early Stage 3 where stiffness dominates.
Shoulder joint capsule distended with steroid, local anaesthetic, and saline under ultrasound guidance. Stretches and may rupture the contracted capsule.
Published cohort data shows significant ROM improvement. Most effective when capsule is still distensible.
Stage 2 to Stage 3 where physiotherapy has plateaued over 6 to 12 months.
Under anaesthesia, the shoulder is manipulated to break adhesions. Done in the operating theatre. Immediate ROM gain.
A 2024 meta-analysis found similar outcomes between MUA and arthroscopic capsular release for resistant frozen shoulder.
Stage 2 to Stage 3 after 12 to 18 months of failed conservative treatment. Preferred in diabetic patients.
Keyhole surgery. The contracted capsule is released with an arthroscope. Physiotherapy begins the following day.
255-patient series at 5.6-year follow-up: significant improvement in all groups. No recurrence at 5 years.
Important note on injections
All steroid and hydrodilatation injections at Medinity Hospital, Gomti Nagar, are performed under ultrasound guidance where clinically appropriate. Blind shoulder injections miss the joint space in 30 to 50% of cases in published studies. Ultrasound guidance maximises accuracy and effectiveness.
Consultation
Need a frozen shoulder treatment plan in Lucknow?
CP-221, Hahnemann Medinity Hospital Road, Gomti Nagar, Lucknow 226010 · Walk-in OPD · 24/7 emergency
How long does frozen shoulder take to heal? An honest timeline
2 to 4 years total from onset to resolution. Most cases resolve, but some have persistent restriction at 7 to 10 years.
12 to 18 months to significant improvement.
Faster pain resolution in weeks rather than months for the pain component. Does not dramatically shorten total disease duration.
Significant ROM improvement within 4 to 8 weeks of the procedure. Physiotherapy must continue to consolidate the gain.
Immediate post-operative ROM improvement. Near-full range of motion by 3 to 6 months post-surgery.
Expect 6 to 12 months longer than non-diabetic frozen shoulder at every stage. Blood glucose optimisation improves outcomes.
Exercises you can do at home and what to avoid without a physiotherapist
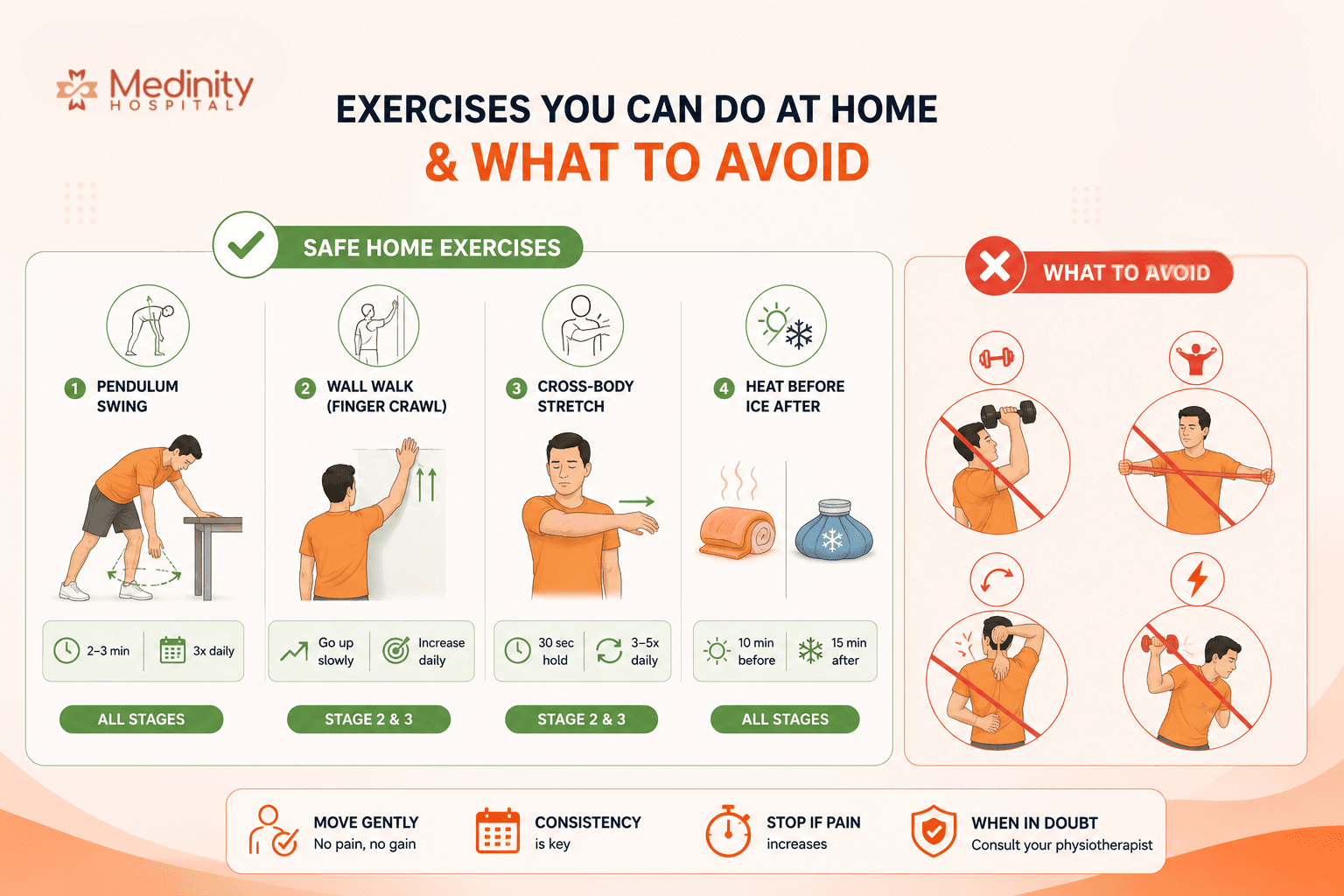
All stages, especially Stage 1 and 2
Lean forward, good arm supported on table. Let affected arm hang and swing in small circles using gravity, not muscle effort. 2 to 3 minutes, 3 times daily.
Stage 2 and 3
Stand facing wall. Walk fingertips upward slowly to point of mild discomfort. Mark height. Try to go slightly higher daily.
Stage 2 and 3
Use good arm to gently pull affected arm across body at shoulder height. Hold 30 seconds. Repeat 3 to 5 times daily. Gentle pull sensation only.
All stages
Warm towel 10 minutes before exercises. Ice 15 minutes after. Heat relaxes capsule. Ice reduces post-exercise inflammation. Never heat a swollen inflamed shoulder.
What To Avoid
- ✗ Aggressive forced stretching at any stage: inflames the capsule and extends recovery
- ✗ Overhead weight training while the shoulder is frozen
- ✗ Traction pulley systems: associated with worsening in Stage 1
- ✗ Deep massage directly into the shoulder joint
- ✗ Exercising through sharp pain
Can frozen shoulder be prevented? What you can actually do to reduce your risk
Frozen shoulder cannot always be prevented, particularly the idiopathic type that develops spontaneously in middle-aged adults with no trigger. However, several known risk factors and precipitating causes are controllable. Here is what genuinely reduces the risk:
Anyone with a shoulder sprain, minor rotator cuff injury, or post-operative shoulder
Begin gentle shoulder range-of-motion exercises (pendulum exercises) within the first 48 to 72 hours of injury, unless specifically contraindicated by the surgeon.
The shoulder capsule starts contracting rapidly during immobilisation. Early movement prevents the inflammatory and fibrotic cascade that initiates frozen shoulder.
Patients treated with slings for wrist, elbow, or other arm injuries
If a sling is prescribed for another arm condition, ask the treating doctor whether shoulder movement is safe. Perform shoulder circles and pendulum exercises regularly if the shoulder itself is not injured.
Frozen shoulder after arm injuries is directly related to shoulder immobilisation duration. Many patients develop it preventably while wearing slings for wrist fractures.
Patients with known diabetes
Keep HbA1c below 7. Monitor blood glucose regularly. Regular follow-up with your physician. If shoulder stiffness develops, do not wait to see an orthopaedic specialist.
Diabetic frozen shoulder is significantly more severe and harder to treat. Good glucose control reduces the severity of the condition if it does develop and improves the response to treatment.
Patients with hypothyroidism or hyperthyroidism
Ensure thyroid hormone levels are in the normal range with your physician. Do not delay thyroid treatment.
Both thyroid disorders are independently associated with frozen shoulder risk. Optimised thyroid function reduces the risk.
Patients who have had shoulder surgery, rotator cuff repair, or arthroscopy
Physiotherapy should begin as soon as the surgeon permits after shoulder surgery. Delayed mobilisation post-operatively is a well-established trigger for frozen shoulder.
Post-surgical frozen shoulder is common, particularly after rotator cuff repair where the arm is immobilised during healing. Early supervised physiotherapy prevents this complication.
All adults over 40, particularly those with diabetes or thyroid conditions
Maintain shoulder range of motion with regular stretching. Avoid prolonged positions with the arm immobile. If stiffness develops, seek assessment within 4 to 6 weeks rather than waiting months.
Frozen shoulder progresses faster when untreated. Seeking assessment early when symptoms first appear gives the best chance of treatment in Stage 1, where outcomes are fastest.
The most preventable frozen shoulder in Lucknow
Post-injury frozen shoulder in patients who are given a sling and told to rest the arm completely for weeks without shoulder mobilisation is entirely preventable. If you or a family member has been given a sling for a wrist or elbow injury in Lucknow, ask the treating doctor specifically whether shoulder range-of-motion exercises should be started. A simple daily pendulum exercise takes two minutes and can prevent months of shoulder stiffness.
Frozen shoulder treatment cost in Lucknow: what determines the price?
Cost is one of the first questions patients ask after a frozen shoulder diagnosis. Here is a transparent framework for what treatment costs in Lucknow in 2025, and what factors influence the final amount:
₹500 to ₹1,500
Often not covered as a standalone outpatient fee
First consultation includes examination and diagnosis. Written treatment plan provided.
₹300 to ₹600 at NABL-accredited centre
Often covered as a diagnostic investigation
Usually done at first visit. Available at Medinity's NABL diagnostics, Gomti Nagar.
₹600 to ₹1,500
Often covered if clinically indicated
Used for diagnosis and to guide injections. Higher accuracy than clinical landmarks alone.
₹4,000 to ₹9,000 depending on centre
Often covered when clinically indicated and pre-authorised
Needed when diagnosis is uncertain or rotator cuff pathology needs to be excluded.
₹1,000 to ₹3,000 including consultation and injection
Some policies cover therapeutic injections
Steroid itself is inexpensive. The cost includes guidance under ultrasound and the consultation component.
₹3,000 to ₹8,000 depending on volume of procedure and medications used
Varies by insurer. Pre-authorise before the procedure
Single procedure, often with significant same-week improvement. Physiotherapy must continue after.
₹400 to ₹800 per session at a qualified centre
Rarely covered for outpatient physiotherapy in most policies
Most Stage 2 patients need 15 to 25 sessions over 3 to 4 months. Medinity Hospital has an integrated physiotherapy department.
₹60,000 to ₹1,50,000 depending on hospital and implant/equipment used
Most major insurance policies cover surgical treatment for frozen shoulder when medically indicated
Includes anaesthesia, single-night hospital stay, and post-operative care. The most definitive treatment for resistant cases.
Transparent Pricing at Medinity Hospital
Medinity Hospital provides a written, itemised cost estimate before any procedure or surgical intervention. To receive a specific cost estimate based on your stage, severity, and insurance situation, call +91 94540 99331 or book a consultation with Dr. R.P. Singh at Gomti Nagar, Lucknow.
Consultation
Want a written cost estimate for your frozen shoulder treatment?
CP-221, Hahnemann Medinity Hospital Road, Gomti Nagar, Lucknow 226010 · Walk-in OPD · 24/7 emergency
Why patients in Lucknow choose Medinity Hospital for frozen shoulder
- Dr. R.P. Singh: MS Ortho (Gold Medalist), Fellowship Joint Reconstruction, USA and Germany
- 20+ years of orthopaedic practice, 2,000+ surgeries performed
- Accurate stage-based diagnosis before starting any treatment
- Steroid and hydrodilatation injections under ultrasound guidance
- Integrated physiotherapy at the same Gomti Nagar campus
- NABH-accredited hospital | NABL-accredited diagnostics
- 4.8-star rating from 246+ verified Google reviews
- Serving patients from Lucknow, Sitapur, Hardoi, Barabanki, Raebareli, Kanpur and across Uttar Pradesh
Help centre
Frequently asked questions
The key difference is passive movement. In frozen shoulder, both active movement (you moving it) and passive movement (the doctor moving it) are equally restricted. In a rotator cuff tear, passive movement is usually preserved but active movement is weak or painful. A clinical examination with ultrasound or MRI will distinguish the two accurately.
Stage 1 (Freezing): pain is dominant, often severe at night, stiffness is beginning. Stage 2 (Frozen): pain has reduced but the shoulder is very stiff and restricted in all directions. Stage 3 (Thawing): stiffness is gradually improving month by month. Staging requires clinical examination by a specialist. Dr. R.P. Singh stages every frozen shoulder patient at the first assessment at Medinity Hospital, Lucknow.
In most cases, yes, eventually. However, the natural history involves 2 to 4 years of significant shoulder restriction. Appropriate treatment matched to the correct stage significantly shortens this timeline and prevents the muscle wasting and psychological burden of years of untreated pain and stiffness.
About 10 to 20% of patients develop frozen shoulder in the other shoulder, typically 1 to 5 years later. In diabetic patients, bilateral involvement is significantly more common. The second shoulder rarely develops it simultaneously.
Night pain is a characteristic feature of Stage 1. When lying down, the inflamed contracting capsule is under gentle but continuous tension. As the condition progresses to Stage 2, inflammatory pain typically reduces even though daytime stiffness worsens.
Physiotherapy must be matched to the correct stage. In Stage 1, gentle physiotherapy alongside pain management is appropriate. Aggressive stretching in Stage 1 worsens the condition. In Stage 2, structured physiotherapy is the cornerstone of treatment StatPearls 2023. All frozen shoulder patients at Medinity Hospital receive a stage-specific physiotherapy programme in the integrated physio department on the same Gomti Nagar campus.
Hydrodilatation involves injecting a mixture of steroid, local anaesthetic, and saline into the shoulder joint under ultrasound guidance. The fluid distends and stretches the contracted capsule. It is most effective in Stage 2. Published cohort studies show significant improvement in range of motion in the weeks following the procedure.
Surgery is considered when non-surgical treatment has been genuinely tried for 12 to 18 months without adequate recovery. Arthroscopic capsular release is the surgical option of choice. A 255-patient series at 5.6 years showed excellent long-term outcomes with no recurrence.
Yes. Diabetic patients have a 10 to 20% lifetime incidence compared to 2 to 5% in the general population, a 2 to 3 times higher risk (BMJ Open 2023). Diabetic frozen shoulder is more severe, more resistant to treatment, lasts longer, and is more likely to be bilateral.
Some exercises are appropriate at home but the wrong exercises at the wrong stage can worsen the condition. Safe home exercises include pendulum swings, wall walking, and cross-body stretches for Stage 2 and Stage 3. In Stage 1, only the gentlest pendulum exercises are appropriate. Aggressive stretching should only be done under physiotherapist supervision.
Most Stage 2 patients need supervised physiotherapy for 3 to 6 months. Home exercises should continue throughout. Total recovery with good physiotherapy engagement takes 12 to 18 months. This compares to 2 to 4 years without treatment.
Recurrence in the same shoulder is rare. After arthroscopic capsular release, the 255-patient series showed no recurrence at 5 years. About 10 to 20% of patients develop it subsequently in the other shoulder.
Costs range from consultation fees and X-rays at the lower end, through ultrasound-guided injections (₹1,000 to ₹3,000), hydrodilatation (₹3,000 to ₹8,000), and physiotherapy sessions (₹400 to ₹800 each), to arthroscopic capsular release (₹60,000 to ₹1,50,000) for surgical cases. Most major insurance policies cover surgery when medically indicated. Medinity Hospital provides a written cost estimate before any procedure. Call +91 94540 99331.
Yes. A 2023 meta-analysis (Chuang et al.) confirmed a significant association between thyroid disorders and frozen shoulder. Patients with unexplained frozen shoulder should have thyroid function tested. Optimising thyroid levels may improve treatment response.
Frozen shoulder should be assessed by an orthopaedic surgeon who can accurately stage the condition and recommend the right treatment. Dr. R.P. Singh at Medinity Hospital, Gomti Nagar, Lucknow, is an MS Ortho Gold Medalist with fellowship training from the USA and Germany who performs accurate stage-based diagnosis, ultrasound-guided injections, and arthroscopic capsular release for resistant cases. Call +91 94540 99331.
Most comfortable is lying on the back with the affected arm supported on a pillow at the side in a neutral position. Lying on the affected shoulder should be avoided. A small folded towel under the armpit of the affected side can reduce tension on the capsule during sleep.

About the author
Dr. R.P. Singh
MS Ortho (Gold Medalist) · Fellowship Joint Reconstruction (USA, Germany) · Senior Orthopaedic Surgeon
- 20+ years experience
- 2,000+ surgeries
- Partial & total knee replacement
Dr. R.P. Singh leads orthopaedics at Medinity Hospital, Gomti Nagar. He specialises in both joint preservation and replacement, bringing international, evidence-based surgical standards to Lucknow.
View full profile & credentials