Quick answer: what is the difference between a PCL tear and an MCL tear?
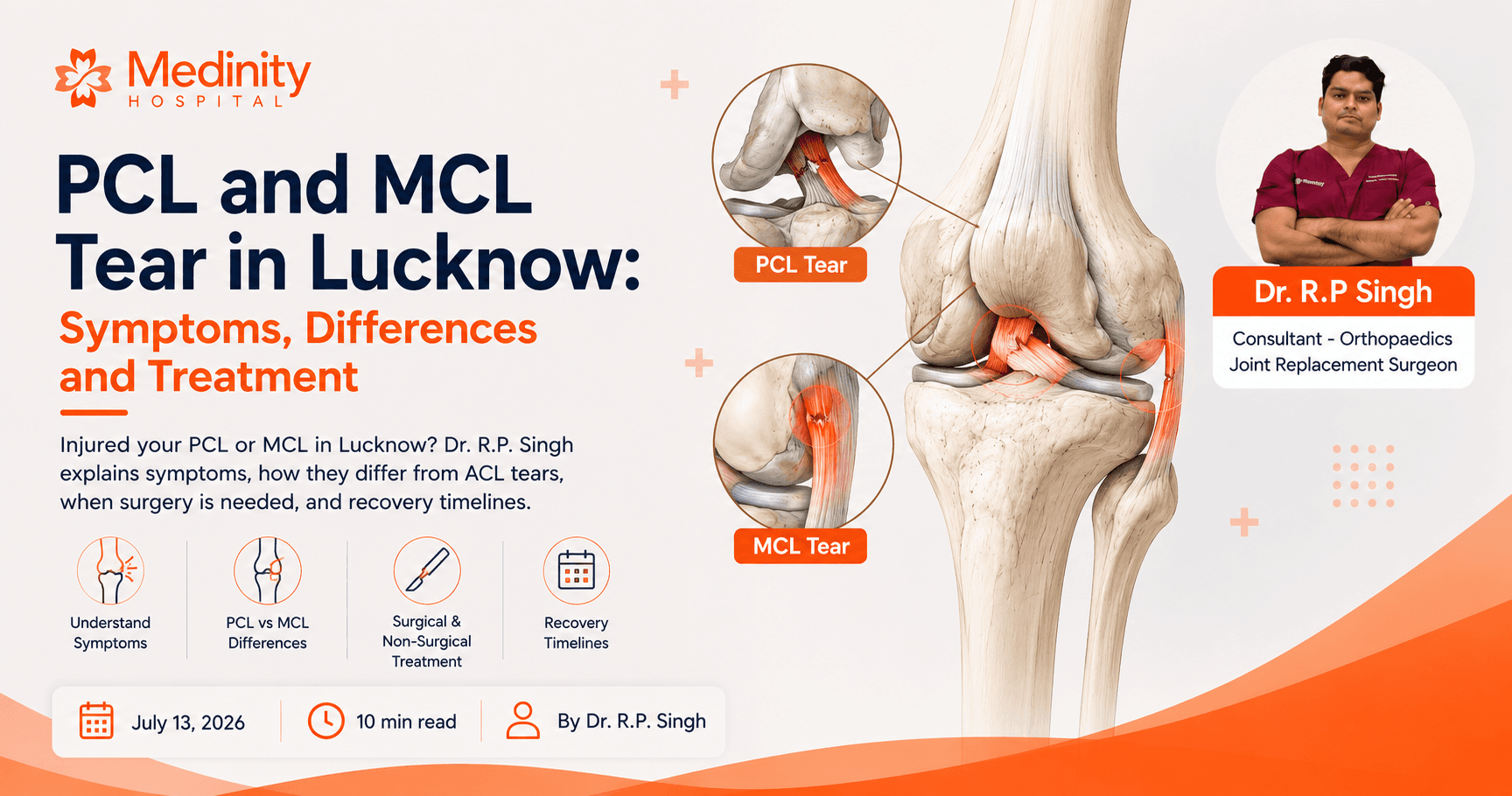
The PCL (posterior cruciate ligament) runs inside the knee and prevents the shin bone from shifting backward. It is torn by a direct blow to the front of the knee, typically in road accidents or contact sports. The MCL (medial collateral ligament) runs along the inner side of the knee and resists inward buckling forces. It is the most commonly torn knee ligament, making up approximately 40% of all knee ligament injuries. Most MCL tears heal without surgery with bracing and physiotherapy. PCL tears are more complex: Grade 1 and 2 often heal non-surgically, while Grade 3 PCL tears in active patients usually require surgical reconstruction.
Knee ligament injuries are not all the same. Most people in Lucknow have heard of the ACL, but the PCL and MCL are just as important and far more commonly misunderstood. Knowing which ligament you have injured is the first step toward the right treatment and a faster return to sport.
Dr. R.P. Singh, sports injury specialist in Lucknow and Senior Orthopaedic Surgeon at Medinity Hospital, Gomti Nagar, regularly treats ligament injuries in cricket players, kabaddi players, football players, and accident patients from across Lucknow, Sitapur, Hardoi, Barabanki, and Raebareli. This article explains what the PCL and MCL are, how to identify which one you may have injured, and what the most appropriate treatment is for each.
What is the PCL and what is the MCL: a simple explanation
Your knee has four main ligaments. Think of them as the ropes that hold the knee joint together and stop the bones from moving in directions they should not move.

Inside the knee, running diagonally from the back of the femur (thigh bone) to the back of the tibia (shin bone). It is the largest and strongest of the four knee ligaments.
Prevents the shin bone (tibia) from shifting backward under the thigh bone. Works with the ACL to keep the knee stable during forward and backward movements.
A direct blow to the front of the bent knee: dashboard injuries in road accidents, landing on the front of the knee in cricket or football, or a hard fall on the knee with the foot pointed downward.
Along the inner side of the knee, running from the femur to the tibia. It is 8 to 10 centimetres in length. It is not inside the joint like the ACL and PCL.
Prevents the knee from bending inward (valgus buckling). Provides side-to-side stability on the medial (inner) side. MCL injuries are the most common of all knee ligament injuries, accounting for approximately 40% of all cases.
A force to the outer side of the knee with the foot planted, pushing the knee inward. Common in football when an opposing player falls into your leg, or in kabaddi and wrestling.
Inside the knee, crossing the PCL in an X-pattern.
Prevents the shin bone from shifting forward. Provides rotational stability. Most commonly known knee ligament.
Planting the foot and changing direction rapidly. Landing awkwardly from a jump. Most common in cricket fielding, football, and badminton.
Along the outer side of the knee.
Prevents the knee from bending outward (varus buckling).
Less common than MCL. Typically injured by a force to the inner side of the knee pushing outward.
How PCL and MCL tears happen: common sports and accidents in Lucknow
PCL and MCL tears happen through very different mechanisms, which is one reason they are often confused with each other in the first days after injury.
A direct impact to the front of the bent knee. The shin bone is driven backward with force.
A valgus (inward buckling) force to the knee with the foot planted. Someone or something hits the outer side of the knee.
Very common PCL mechanism. Dashboarding: the front of the knee hits the dashboard when the knee is bent.
Less common than PCL from accidents, but possible when the side of the knee is struck.
Cricket: diving to stop the ball and landing on the front of the knee. Football: tackles where the knee is struck head-on.
Football: opponent falls into the outer side of the leg. Kabaddi: being tackled with the knee buckling inward. Wrestling and contact sports.
Less common with PCL tears than ACL tears. Many PCL injuries do not produce an audible pop.
A pop or crack is felt when the MCL tears. The knee may feel unstable immediately.
Often yes, especially Grade 1 and 2 PCL tears. Grade 3 may cause significant instability.
Usually yes for Grade 1 and 2 MCL tears. Grade 3 tears cause significant instability and difficulty weight-bearing.
PCL tears very commonly occur alongside other injuries: MCL, ACL, meniscus, or posterolateral corner damage. An isolated PCL tear is less common than combined injury.
MCL Grade 3 tears are frequently associated with ACL tears. This combination is sometimes called the 'unhappy triad' when combined with a meniscus tear.
PCL injuries in Lucknow: road accidents are a major cause
Dr. R.P. Singh sees PCL injuries from road accidents at Medinity Hospital at a significantly higher rate than sports-related PCL tears. When someone brakes suddenly and the knee is hit against the dashboard in a bent position, the shin bone is driven directly backward, which is the exact mechanism that tears the PCL. Any patient with knee pain and instability after a road accident should have a PCL specifically examined, not just X-rays to rule out fracture.
Consultation
Knee injury from a sports collision or accident in Lucknow? Book an assessment today.
CP-221, Hahnemann Medinity Hospital Road, Gomti Nagar, Lucknow 226010 · Walk-in OPD · 24/7 emergency
PCL tear symptoms versus MCL tear symptoms: how to tell the difference
The symptoms overlap significantly, which is why clinical examination and MRI are both needed for an accurate diagnosis. However, there are distinguishing features that point toward one ligament over the other:

Diffuse knee pain, often felt at the back of the knee. Can feel deep inside the joint.
Specifically on the inner (medial) side of the knee, along the joint line. Tenderness directly over the MCL itself, not inside the joint.
Knee pain is present in both. Location helps differentiate.
Swelling tends to fill the entire joint (joint effusion). Can be significant within hours of a severe injury.
Swelling is more localised to the inner side of the knee rather than filling the whole joint. This is an important distinguishing feature from ACL tears.
Both cause swelling. PCL swelling is more diffuse; MCL swelling is more localised.
Knee feels like it may give way during forward activities, going downstairs, or when the knee is bent under load. The tibia may sag backward visibly on examination (posterior sag sign).
Knee feels like it may buckle inward when walking sideways, pivoting, or when weight is placed on the inner side of the joint.
Both cause some instability, but the direction of instability differs.
More common with PCL than other ligaments. Many PCL injuries do not produce a pop or crack.
A pop or crack is commonly felt at the moment of MCL injury.
A pop usually means ligament fibres have failed. Absence of pop is more common with PCL.
Worse going downstairs, deep knee bending, squatting. Loading the knee in flexion puts the PCL under stress.
Worse with any sideways movement or activity that stresses the inner knee. Running and cutting movements.
Both are painful during most sports activities.
Positive: when lying with the knee bent to 90 degrees, the tibia visibly sags backward compared to the other leg. This is a key clinical sign of PCL disruption.
Negative: the tibia does not sag backward in MCL injuries.
Specific to PCL injury.
The key clinical tests used at Medinity Hospital
Dr. R.P. Singh uses three specific tests to assess PCL and MCL injuries. For the PCL: the posterior drawer test (pushing the tibia backward with the knee bent to 90 degrees) and the posterior sag sign. For the MCL: the valgus stress test at 0 degrees and 30 degrees of knee flexion. Laxity at 30 degrees but not at 0 degrees usually indicates an isolated MCL injury. Laxity at both 0 and 30 degrees suggests injury to additional structures. These clinical tests, combined with MRI, give a reliable diagnosis without exploratory surgery.
PCL and MCL injury grades: how severity determines treatment
Both PCL and MCL injuries are graded by severity. The grade is the single most important factor in deciding whether surgery is needed.
MCL injury grades (Cleveland Clinic 2025):
- Fibres torn: Less than 10% of fibres torn
- Stability: Knee still stable
- Pain: Some tenderness and mild pain on inner knee
- Fibres torn: Partial tear of the MCL
- Stability: Knee loose when tested by hand
- Pain: Intense pain and tenderness on inner side
- Fibres torn: Complete tear of all MCL fibres
- Stability: Knee very unstable and loose
- Pain: Intense pain, may be associated with ACL tear
PCL injury grades:
- Fibres torn: Partial tear present
- Stability: Knee stable
- Pain: Mild pain, can usually bear weight
- Fibres torn: Partial tear, ligament feels loose
- Stability: Some laxity on testing
- Pain: Moderate pain, knee feels unreliable
- Fibres torn: Complete tear, knee unstable
- Stability: Significant posterior laxity
- Pain: Significant pain, posterior sag sign positive
- Fibres torn: PCL plus another ligament also injured
- Stability: Complex instability
- Pain: Often involves ACL, MCL, or posterolateral corner
PCL and MCL tear versus ACL tear: which is more serious and why?
Patients who know they have a knee ligament injury almost always ask this question. Here is the honest clinical comparison:
Most commonly discussed ligament injury. Very common in cricket, football, kabaddi.
Less than 20% of knee ligament injuries. Often occurs with other injuries in road accidents and contact sports.
Most common knee ligament injury. Approximately 40% of all knee ligament injuries (Cleveland Clinic).
Very common. Most patients describe a definite pop.
Less common. Many PCL injuries are silent.
Common. Patients often feel or hear a crack at the inner knee.
Immediate, significant joint effusion. Knee balloons within hours.
Moderate to significant, fills the joint.
More localised to the inner side. Does not usually fill the whole joint.
Knee gives way with cutting, pivoting, and landing. Rotational instability is dominant.
Knee gives way going downstairs or with deep bending. Posterior instability.
Knee buckles inward. Medial instability.
Grade 1 and 2: possible with physio. Grade 3 in active patients: surgery almost always recommended.
Grade 1 and 2: often heal with physio and bracing. Grade 3: controversial, but trend toward surgery in active patients.
Grade 1 and 2: almost always heal without surgery. Grade 3: usually heals without surgery, but may need surgery if associated <a href="/blog/acl-cricketers-lucknow/" class="text-[#C84B31] font-semibold hover:underline">ACL</a> tear is present.
ACL reconstruction using hamstring or patellar tendon graft. 6 to 9 month recovery.
PCL reconstruction. Complex. 6 to 12 month recovery. Longer than ACL.
MCL repair (end-to-end suture) or reconstruction. 4 to 6 month return to sport.
Grade 1-2: 6 to 12 weeks. Grade 3 without surgery: rarely satisfactory in active patients.
Grade 1-2: 4 to 12 weeks. Grade 3: 3 to 6 months, with surgery potentially 6 to 12 months.
Grade 1: 2 to 4 weeks. Grade 2: 4 to 8 weeks. Grade 3: 4 to 6 months.
The MCL is the ligament most likely to heal well without surgery among the four major knee ligaments. The PCL is the strongest ligament in the knee and can also heal non-surgically in many cases. The ACL has very poor blood supply and very rarely heals without surgery in active patients. This is why ACL surgery recommendations are more consistent than for MCL and PCL.
Consultation
Unsure which knee ligament is injured? Get a proper diagnosis before starting treatment.
CP-221, Hahnemann Medinity Hospital Road, Gomti Nagar, Lucknow 226010 · Walk-in OPD · 24/7 emergency
Does a PCL or MCL tear require surgery? The decision framework
This is the question every ligament injury patient asks. Here is the honest framework Dr. R.P. Singh uses at Medinity Hospital, based on current orthopaedic evidence:
No
Heals reliably with bracing, rest, and physiotherapy. Surgery is not indicated.
Hinged knee brace, RICE protocol (rest, ice, compression, elevation), physiotherapy starting with quad strengthening. Return to sport in 2 to 4 weeks.
No in most cases
Heals without surgery in the vast majority of patients. Even with significant laxity on examination, the MCL has excellent blood supply and healing potential.
Hinged knee brace for 3 to 6 weeks, progressive physiotherapy, hamstring and quad strengthening. Return to sport in 4 to 8 weeks.
Usually no, unless displaced
Isolated Grade 3 MCL tears can heal conservatively. Surgery is considered when the ligament has pulled away from the bone with a bony fragment (avulsion fracture) or when a significant bony attachment is displaced.
6 weeks in a hinged brace with progressive weight-bearing, then intensive physiotherapy. Return to sport in 4 to 6 months.
Yes, typically
The combination of MCL and ACL tears creates complex instability. The MCL is usually allowed to heal first (6 to 8 weeks) before ACL reconstruction is performed.
Staged approach: MCL heals first, then ACL surgery at 6 to 8 weeks. Full recovery 9 to 12 months.
No in most cases
Grade 1 and 2 PCL tears frequently heal non-surgically with aggressive hamstring rehabilitation. The hamstrings substitute for PCL function.
Physiotherapy focused on hamstring strengthening. Bracing. Avoid activities loading the knee in flexion. Return to sport in 4 to 12 weeks.
Increasingly yes
The trend in recent years has moved toward surgical reconstruction for Grade 3 PCL tears in athletes and active young patients. Non-surgical treatment of Grade 3 PCL tears has an unpredictable outcome and patients who delay surgery often face 6 to 12 months of total downtime anyway.
PCL reconstruction using hamstring tendon graft. 6 to 12 months total recovery. Intensive rehabilitation.
Yes
Complex knee instability involving the PCL and other structures (ACL, MCL, posterolateral corner) almost always requires surgical treatment. These are high-energy injuries, often from road accidents.
Multi-ligament knee reconstruction. Staged or simultaneous depending on the injury pattern. Longest and most complex recovery of any knee ligament injury.
The danger of delaying Grade 3 PCL surgery
A common scenario at Medinity Hospital: a patient with a Grade 3 PCL tear tries non-surgical rehabilitation for 4 to 6 months, does not recover full function, then proceeds to surgery. Total downtime: 12 to 18 months. If the same patient had surgery at 4 to 6 weeks, total downtime would have been 6 to 9 months. For Grade 3 PCL tears in athletes, early specialist assessment and a clear decision (surgery or structured non-surgical rehabilitation) is critical.
Recovery timeline and return to sport: what Dr. R.P. Singh tells his patients
2 to 4 weeks
Surgery rarely needed
2 to 4 weeks
4 to 8 weeks
Surgery rarely needed
6 to 8 weeks
3 to 4 months with full bracing and physio
4 to 6 months if surgery required
4 to 6 months
MCL heals in 6 to 8 weeks, but <a href="/blog/acl-cricketers-lucknow/" class="text-[#C84B31] font-semibold hover:underline">ACL</a> limits sport
9 to 12 months total (staged: MCL first, then ACL surgery)
9 to 12 months
4 to 12 weeks with hamstring rehab
Surgery rarely needed
6 to 12 weeks
4 to 6 months, but outcome unpredictable
Not applicable
Variable, often unsatisfactory in athletes
Not applicable
6 to 12 months
6 to 12 months. Longer than ACL recovery.
Not applicable for Grade 4
12 to 18+ months
12 to 18 months or longer
The single most important principle in ligament injury recovery: do not rush return to sport. Returning before the ligament has healed and before the surrounding muscles are strong enough is the most common reason for re-injury. Dr. R.P. Singh clears patients for return to full sport only when quadriceps and hamstring strength on the injured side is within 90% of the uninjured side and clinical stability is confirmed.
Why athletes and injury patients in Lucknow choose Medinity Hospital for ligament injuries
- Dr. R.P. Singh: MS Ortho (Gold Medalist), Fellowship Sports Injury and Joint Reconstruction, USA and Germany
- 20+ years of orthopaedic practice, 2,000+ surgeries performed
- Clinical PCL-specific tests (posterior drawer, posterior sag) performed at every assessment
- MRI at Medinity's NABL-accredited diagnostics centre on the same visit
- Non-surgical management first, surgery only when clinically indicated
- NABH-accredited hospital | 4.8 stars | 246+ verified reviews
- Patients from Lucknow, Sitapur, Hardoi, Barabanki, Raebareli, Kanpur and across UP
Help centre
Frequently asked questions
PCL tears typically cause diffuse knee pain, swelling throughout the joint, and a feeling of instability when going downstairs or bending the knee deeply. MCL tears cause pain and tenderness specifically on the inner side of the knee, with swelling localised to the inner knee rather than filling the whole joint. The posterior sag sign (tibia drooping backward when the knee is bent to 90 degrees) is specific to PCL injury. An MRI is needed to confirm which ligament is torn and to what extent. Dr. R.P. Singh at Medinity Hospital, Lucknow, performs both clinical tests and arranges MRI at the NABL-accredited lab on the same visit.
Most MCL tears (Grade 1, 2, and many Grade 3) heal without surgery with bracing, rest, and physiotherapy. The MCL has excellent blood supply and healing potential. PCL Grade 1 and 2 tears also frequently heal without surgery with aggressive hamstring rehabilitation. The controversy is with Grade 3 PCL tears in active patients and athletes, where the trend in recent years has shifted toward surgical reconstruction because non-surgical outcomes are often unpredictable for patients wanting to return to sport.
The posterior sag sign is a key clinical test for PCL injury. With the patient lying on their back and the knee bent to approximately 90 degrees, the tibia (shin bone) visibly droops backward compared to the other knee. This backward sagging is caused by the loss of PCL tension that normally holds the tibia forward. A positive posterior sag sign indicates significant PCL disruption. It is one of the first tests Dr. R.P. Singh performs when PCL injury is suspected at Medinity Hospital, Lucknow.
MCL tears cause pain specifically on the inner side of the knee, while ACL tears cause more diffuse knee pain and swelling throughout the joint. MCL tears rarely cause rotational instability (the feeling that the knee might twist and give way) which is characteristic of ACL tears. Crucially, MCL tears almost always heal without surgery, while Grade 3 ACL tears in active patients almost always require surgical reconstruction. This is the most clinically important distinction between the two injuries.
Grade 1 and 2 MCL tears: most patients can walk, though with pain and some difficulty. Grade 3 MCL tears: walking is possible but the knee feels very unstable and insecure. Grade 1 and 2 PCL tears: most patients can walk, often with less immediate difficulty than an ACL tear. Grade 3 PCL tears: walking is possible but the knee may feel unreliable on stairs and slopes. In all cases, a hinged knee brace provides significant support and comfort immediately after injury while formal assessment and MRI are arranged.
A PCL bruise (bone contusion or bone bruise on MRI) means the bone around the PCL has been compressed and shows oedema on MRI, but the PCL ligament fibres themselves are intact. This is technically a Grade 0 or very mild Grade 1 injury. A PCL bruise heals with rest and protected activity within 4 to 8 weeks in most cases. A PCL tear means the ligament fibres have actually been disrupted, which requires more specific management based on the grade. MRI is needed to distinguish the two.
An MRI is strongly recommended for any significant knee injury where ligament damage is suspected. X-rays show bones but not ligaments. An MRI reveals which ligament is torn, the extent of the tear (Grade 1, 2, or 3), whether the bone attachment is avulsed, and whether any associated structures such as the meniscus, cartilage, or other ligaments are also damaged. This information directly determines treatment. At Medinity Hospital, Gomti Nagar, Lucknow, MRI can be arranged at the NABL-accredited diagnostics centre on the same day as the consultation.
For MCL tears, a hinged knee brace with rigid side brackets is recommended. Simple compression sleeves without hinges do not provide sufficient support for significant MCL tears. The hinged brace limits sideways movement while allowing controlled bending and straightening. For PCL tears, a PCL-specific functional brace that limits posterior tibial translation is used in more significant injuries. Dr. R.P. Singh prescribes the appropriate brace type at the initial assessment and adjusts it as recovery progresses.
Grade 1 MCL tears: a brace for 1 to 2 weeks, primarily for comfort and confidence during activity. Grade 2 tears: 3 to 6 weeks of consistent brace use, transitioning to sport-specific activity. Grade 3 tears: 6 to 8 weeks of full bracing before progressive rehabilitation begins. The brace protects the healing ligament from being re-stretched during the critical first weeks of healing. Wearing the brace consistently, especially during any activity, is essential.
Yes, in most cases. PCL reconstruction is considered technically more demanding than ACL reconstruction because the PCL runs deeper in the knee and is positioned closer to critical neurovascular structures. Recovery is also longer, typically 6 to 12 months for PCL versus 6 to 9 months for ACL. This is one reason why the decision to operate on a Grade 3 PCL tear requires careful consideration by an experienced orthopaedic surgeon with specific ligament reconstruction expertise.
Yes. Cricket fielders who dive to stop the ball and land on the front of the knee with the knee bent are at risk of PCL injury. The impact drives the shin bone backward against the PCL. Fast bowlers can also sustain PCL injuries from high-impact falls. In Lucknow, where cricket is played intensively, Dr. R.P. Singh regularly assesses PCL injuries in players from local clubs across Gomti Nagar, Indira Nagar, and surrounding areas.
The "unhappy triad" refers to a classic combination of three knee injuries occurring simultaneously: ACL tear, MCL tear, and medial meniscus tear. This injury pattern is common in sports where the knee receives a valgus (inward buckling) force with simultaneous rotational stress, such as a tackle in football or kabaddi. The combination is called "unhappy" because it involves three structures needing treatment simultaneously. Management of the unhappy triad requires careful planning of which structure to prioritise, and surgery is almost always required for the ACL component.
In the first 1 to 2 weeks: quadriceps sets (tightening the quad without bending the knee), straight leg raises, and ankle pumps for circulation. Weeks 2 to 4: partial weight-bearing with brace, short arc quad exercises, mini squats to 30 degrees. Weeks 4 to 8: progressive quad and hamstring strengthening, balance exercises, cycling at low resistance. The MCL's specific role in medial (inner) stability means medial hamstring strengthening (semitendinosus and semimembranosus) is particularly important. All exercises should be supervised by a physiotherapist, particularly in the early stages.
Dr. R.P. Singh uses two criteria before clearing return to sport at Medinity Hospital, Lucknow. First: the injured side's quadriceps and hamstring strength must be within 90% of the uninjured side on testing. Second: the patient must be able to perform sport-specific movements including running, cutting, and pivoting without pain or instability. For MCL tears, this typically takes 4 to 8 weeks for Grade 1 and 2, and 4 to 6 months for Grade 3. For PCL injuries, it takes 3 to 6 months non-surgically and 6 to 12 months post-surgery.

About the author
Dr. R.P. Singh
MS Ortho (Gold Medalist) · Fellowship Joint Reconstruction (USA, Germany) · Senior Orthopaedic Surgeon
- 20+ years experience
- 2,000+ surgeries
- Partial & total knee replacement
Dr. R.P. Singh leads orthopaedics at Medinity Hospital, Gomti Nagar. He specialises in both joint preservation and replacement, bringing international, evidence-based surgical standards to Lucknow.
View full profile & credentials